Driving along the King’s way
- 29 August 2013
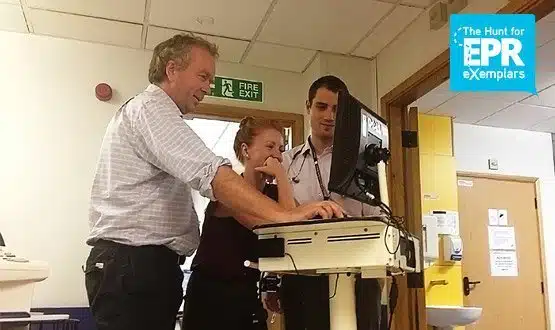
EHI recently joined Dr Jack Barker on a ward round on a general medicine ward at King’s College Hospital in London.
Instead of gathering around a whiteboard or a stack of notes, the consultant in general and respiratory medicine and two junior doctors refer only to a computer screen.
This conveys everything that the consultant, who is also the trust’s chief clinical information officer, and his colleagues need to know about a patient’s condition.
Via the trust’s electronic patient record system, they can review all the tests that have been ordered and the results, medications prescribed and delivered, and all nursing observations from the patient’s stay.
Readings that are out of the ordinary range show up in red so they can be quickly identified. At one point, Dr Barker wants to know if an endoscopy has been ordered; he soon establishes that it is due to be done that afternoon.
One of the junior doctors, Rob, clasps a sheet of paper listing his patients; but he admits this is force of habit from working in other hospitals. He says he never writes on paper at King’s.
The level of digitisation is undoubtedly impressive, although it does put big demands on the trust’s infrastructure and hardware.
Minutes earlier, the hospital corridor was filled with the loud beeping of one of the ‘computers on wheels’, as another junior doctor dragged it towards a power socket for charging.
Battery power is apparently an issue and sockets are in high demand, so the doctor finds herself trapped behind three COWS and a lot of wires, from which she has to untangle herself.
The Hunt for EPR Exemplars
In August, EHI launched ‘The Hunt for EPR Exemplars’ as the next stage in ‘The Big EPR Debate’ that it started in April. The idea is to find trusts that have good IT overall, that are known for their work in particular areas, and that have lessons from which others can learn.
King’s stands out as a candidate to be an EPR Exemplar. It scores highly on a new Digital Clinical Maturity Index developed by EHI’s research arm, EHI Intelligence.
Cited as one of the most advanced trusts in the country by health secretary Jeremy Hunt when he called for the NHS to go ‘paperless’ by 2018, it is thought to be one of just a handful that could already deliver the new Hospital Episode Statistics demanded by NHS England.
It has spent years rolling out e-prescribing and, more recently, has done interesting work on nursing observations with Tactix4.
Still, while being recognised as an exemplar is an honour, it also has its dangers; as illustrated on the ward visit, a trust can have very good systems in place, but things will rarely be perfect.
King’s IT director Colin Sweeney knows this well. “It’s an honour, of course, but it’s dangerous in that the pride comes before a fall,” he says.
“We know our systems aren’t perfect, but if something goes wrong people can say, ‘are they as good as they are being held up to be’?”
Despite these reservations, Sweeney also knows that his trust is seen as being at the forefront of lots of initiatives. “I think we are fairly well advanced compared to lots of organisations,” he says.
“For electronic ordering and results, e-prescribing, and inpatient noting we have been ahead of the game. That said, other people are going to be more advanced in other areas, as that’s where their priority has been.”
Do it, do it again
So what is King’s secret (if it has a secret)? “There’s a culture here that we just get on and do things. We are not afraid to make mistakes. We will try something and if it doesn’t work we will take it out, fix it, and try again,” Sweeney says.
He cites the trust’s e-prescribing deployment in 2004-05. When major problems were discovered, the team decided to stop, take out the system and fix it, and then restart the deployment.
Sweeney also argues that trusts need to keep a close eye on whether users are getting benefits from new systems. These should be clinical benefits that support patient safety and quality, but even Sweeney acknowledges that these are notoriously hard to measure.
Initially, King’s did things like measure how long it took to get batches of tests done using paper forms and the time saving of doing the same thing electronically. These days, it looks more at whether staff adopt the new way of working because it makes their lives easier.
“We’ve certainly never measured the benefits financially. It’s always been about quality of treatment as far as we are concerned, and trying to improve people’s lives,” Sweeney explains.
The trust invests about £10m a year in IT from a turnover of £600m; or about 1.6%. While that’s not a huge amount of money, it’s a lot compared to what some trusts have to invest in technology.
The money supports local developments and configurations of the trust’s EPR that would be very difficult to replicate in some organisations.
However, there are certain lessons about IT adoption that are universal. Sweeney says having support at executive level is crucially important, especially at the beginning of a major EPR project.
“Fifteen years ago, the chief executive and finance director said: ‘We have to this, we need to move forward.’ The finance director said: ‘Don’t say you are going to save money, it’s just something we are going to have to do’ and that philosophy has been carried through,” Sweeney says.
Broadly, he also adheres to the approach to EPR set out in the Information for Health strategy in 1998, which set out a six-level ladder to EPR that trusts were supposed to implement locally, picking their own systems to do it.
When trusts failed to hit targets for reaching the different levels, the government panicked and introduced NPfIT.
But the IfH idea – that first you get a patient administration system, then order communications and results reporting, then e-prescribing, then clinical noting and observations – still has a lot of support within the NHS.
So retro its cool again
King’s has built its IT around an iSoft (now CSC) PAS, iPM, and its clinical software, iCM. For some years, it was an iSoft reference site and it used to get a lot of visitors before NHS Connecting for Health was set up.
During the NPfIT years, it received far less attention. But as NHS mandarins and government ministers began to shift the attention back to local IT, King’s became a focus of interest once again.
The trust bolted inpatient noting onto iCM system in 2009. Anyone and everyone is expected to use the system to record patient information electronically, and that includes specialists visiting from other trusts or units.
The trust still has a set of paper notes for every patient, but they are noticeably thin as 70-80% of information is now recorded and handled on a computer. Much of the paper comes into the hospital from the outside and needs to be scanned.
King’s is soon embarking on a scanning project to deal with this influx as well as to make historical paper notes available digitally. It is also working on creating e-forms to replace the multitude of paper forms still in use.
Nursing observations system WardWare is also being used on about 50% of wards as part of a steady roll-out. Nurses use iPods to record patient vital signs and calculate National Early Warning Scores.
Back on the general medicine ward, nurse sister Pat Ikhena says she finds the allergies flag at the top of patient records particularly useful. When she is doing a drug round, she will log in to see what a patient needs at what time and whether it has been dispensed.
“If a doctor is in another part of the hospital they can access the system and review the patient and add anything such as medication changes,” she explains.
Outreach teams also have access to WardWare. This means a team can suddenly appear to check on a patient that they have identified as deteriorating, Ikhena adds.
Measuring the benefits
Dr Barker says that while it is very hard to measure benefits, academic papers suggest that the trust’s level of IT adoption has helped it to meet various targets, such as venous thromboembolism assessments.
However, he acknowledges that some things will take longer to do electronically than they take to do on paper. In these cases, clinicians have to be convinced that the improvement in quality is worth the effort.
“There are costs at the time you are actually recording it from doing it on the computer, but you get more quality when using the computer.”
Dr Barker believes that King’s strategy of doing a lot of work internally also helps to keep the IT connected to the user. It means that if something doesn’t work, a clinician can go directly to the people responsible.
“Local ownership has been really important to us. Colin’s run a very good department and managed to retain quite a lot of good resource,” he comments.
Just keeping at it is also important. Six or seven years ago, King’s staff were very nervous about making significant changes.
“It was tough. We had a lot of complaints. Now it’s much quieter because I think we have got their confidence a bit more,” Dr Barker says.
Getting through the hard times means having people who will “hold their nerve and not crumble” under opposition, he adds; claiming, cheerfully, that clinicians like himself are the ideal people to do this because “they have a brilliant propensity to bullsh*t.”
On the other hand, it means having people around who can say “this is just wrong and it doesn’t make sense” if something really needs changing. And Dr Barker has done his fair share of that, as well, on the way to getting King’s where it is.
King’s College Hospital NHS Foundation Trust: the journey to date
| 1999 | Initial pilot of iCM |
| 2002 | Order communications |
| 2004 | Picture archiving and communications system |
| 2008-10 | E-prescribing |
| 2009-10 | Inpatient noting |
| 2012-present | Nursing observations |
| Future projects – e-forms and scanning | |
| IT spend – £10m a year, or approximately 1.6% of the trust’s turnover | |